A one-year recovery trip report for a torn ACL + Meniscus.
In August 2020, after a pretty amazing summer of climbing, I tore my ACL and meniscus in my right knee, while descending from a climb in Rocky Mountain National Park. The injury was bad enough and the terrain rugged enough that I had to be helicopter evacuated off the mountain. A couple of weeks later I got surgery to repair my ACL and meniscus. Due to combination of a skilled surgeon and my dedication to physio, less than 4 months from surgery I was (carefully) climbing multipitch routes and hiking with a heavy pack, and back to full action about 8 months from surgery, ready to hit the summer climbing season strong. This page documents the recovery process.
Trip Report
CLICK ON THE SECTION HEADER TO DROPDOWN THE CONTENT
(Some of the following is copy/pasted from my Goldfinger trip report where I give the original accident report.)
In August 2020, while jumping from one boulder to the next coming down from the summit of Arrowhead, my knee buckled underneath me and it sounded as if a small explosion went off in my knee....$#!&....
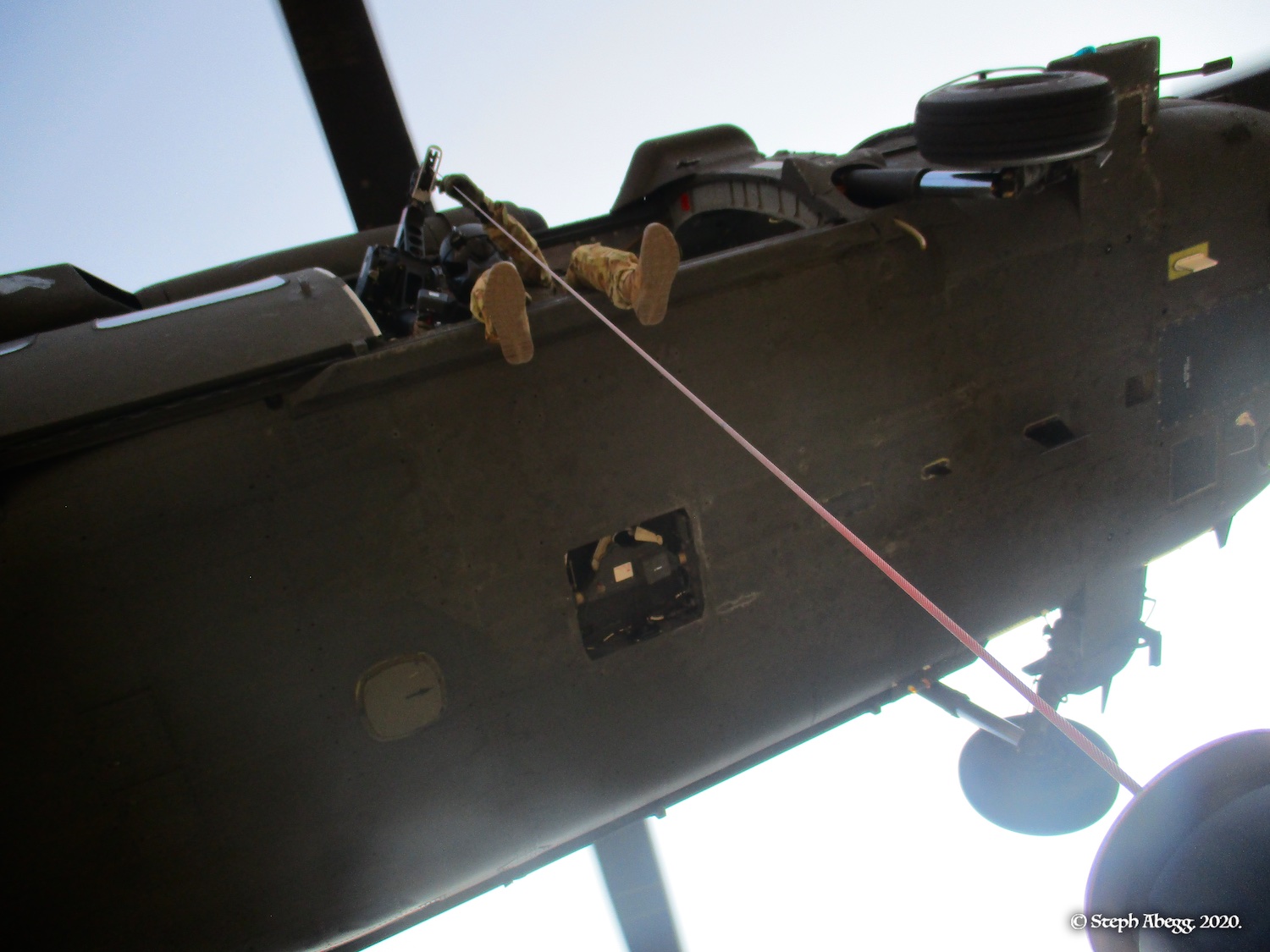
I tried to stand up, but my knee buckled and a wave of excruciating pain shot through my leg. It was pretty clear that my knee would not support my weight. Nate and I had to make a decision: Do we try to self-rescue (which would involve me crawling a couple of miles of quite rugged terrain to the trail and then Nate piggy-backing me out from there) or do we call the Rocky Mountain National Park Search and Rescue team while we still had cell service? The summit of Arrowhead gets a bit of cell service (Verizon at least) and ever since my life-(or at least leg-)saving phone call for a serious tib/fib injury in 2010, I always bring my phone on a climb. Both Nate and I lean towards self-rescue if possible. I tried to stand up again, and again my leg buckled and and I yelped in pain. Okay, maybe I was less ambulatory than I thought. We decided to make the call to SAR. We wrapped my leg in my small climbing pack to attempt to stabilize it. I began to sideways crawl and butt-scoot along the summit ridge towards the rappel route while Nate passed on the necessary details to the SAR team (i.e. my status, our plan to self-rescue to upper McHenrys basin, and the approximate location of our bivy site there). What is normally a casual 10-15 minute romp from the summit to the top of the rap route became a rather butt-bruising 2 hour scoot. Once we arrived at the rappels, Nate lowered me while I used my good leg and two hands to keep my knee from hitting the rock. From the base of the two rappels Nate belayed me for another rope length while I butt-scooted down the steep granite slabs towards the bivy cave where we had stayed the night before. The entire descent from the summit, which typically would have taken under an hour, took just over 3 hours (which actually isn't too bad considering the circumstances). We re-established ourselves at our bivy site and waited for the SAR team to arrive. I wolfed down a handful of expired pain meds and tried to study some math and Nate tried to read a book. The 3-person ground SAR team arrived a few hours later. The medic assessed my condition and splinted my knee, and then the team assessed the best means to get me out. The main means of rescue in RMNP are foot, horse, helicopter land and load, and helicopter hoist. Due to the rugged location and my non-ambulatory status, the SAR team deemed it best to request assistance from a Colorado National Guard helicopter from Buckley Air Force Base to extricate me via a hoist operation, using a winch operated cable. It was too late in the day for the chopper to come that evening, so we all settled in for the night. The Blackhawk chopper arrived as scheduled the next morning at 8:00am for their first recon loop. They had to make two attempts to successfully lower a rescue personnel, who strapped me into a screamer suit, grabbed the swinging 100-foot cable, clipped us both in along with my pack, and signaled the chopper to begin winching us up as it flew off. Eight minutes later we touched down at Upper Beaver Meadows. Nate had hiked out early and was there to meet us. Part of the reason for this was to avoid the costly unnecessary ambulance ride, but the best part was seeing a familiar and friendly face. I made some calls to my insurance company to make sure the Estes Park Hospital was in-network, and after confirming it was, Nate dropped me off at the ER for the day, telling me to call him when I was ready to be picked up. I couldn't ask for a better friend and climbing partner.
Once more, I want to express my gratitude to the Rocky Mountain National Park Search and Rescue Team, the Colorado National Guard helicopter team, and most especially to Nate for executing this rescue with efficiency, precision, and compassion.
Accident/Rescue Timeline
- Hurt knee near summit: 12:05 pm, Thursday, August 20 - Phone call to SAR: 12:25 pm - Top of rappels: 2:03 pm - Back at Bivy: 3:20 pm - SAR arrives: 6:48 pm - Helicopter pick-up: 8:23 am, Friday, August 21 - Upper Beaver Meadows: 8:31 am - Estes Park Hospital: 11:20 am
Photos
Photos from the successful evacuation below.
Photos:
Photo descriptions:
DAYS
1&2
AUG 20&21
2020
ACCIDENT &
RESCUE
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
1. We wrapped my leg in a pack and I crawled from the summit to the first rappel anchor.
2. We set my hot pink rope on a boulder to help the Search and Rescue Team find us.
3. I tried to study a bit as we waited for SAR to arrive.
4. The ground SAR team.
5. Split and rope.
6. The ground SAR team.
7. Making radio contact with the helicopter.
8. The view of Chiefs Head must be amazing.
9. Blackhawk helicopter. 10-22. The hoist.
23. Safe in the chopper. 24. In the hospital filling out some paperwork....getting ready for some bad news....
The ER at the Estes Park Hospital was characteristically empty when I arrived, and a nurse rushed to meet me with a wheelchair as soon as she saw me hop out of Nate's truck. I spent the next several hours filling out forms, being prodded, getting x-rays and an MRI, talking with the attending ER doctor, scheduling some surgeries, and texting my parents in the interim periods. The news was not good (bold are the main ones requiring surgery and long-term recovery):
Fracture of the posterior aspect of the lateral tibial plateau, predominantly a nonarticular cortical depression fracture, but there is also an osterchondral component involving the posterior articular surface.
Cartilage defect (approximately 12x4 mm) within the posterior lateral tibial plateau at the osterochondral fracture site.
Torn proximal ACL.
MCL and FCL sprains. No high-grade tear identified.
Large, displaced bucket-handle tear of the lateral meniscus with the handle displaced into the intercondylar notch, slightly greater anteriorly.
Vertical longitudinal tear of the peripheral posterior horn of the medial meniscus (ramp lesion).
Large hemarthrosis with posterior capsular tear and extensive hemorrhage and edema within the popliteal fossa.
Bone contusion of the anterior aspect o the tibial plateau involving the medial and lateral aspect and a smaller bone contusion of the posterior medial tibial plateau. Small osterochondral impaction fracture of the anterolateral femoral condyle at the condylopatellar sulcus and bone contusion of the upper peripheral lateral femoral condyle.
High-grade partial thickness tear of the mid substance of the quadriceps tendon at its patellar insertion measuring approximately 13 mm in length. The peripheral fibers, lateral greater than medial, are intact. (Note: This quadriceps tendon damage was likely a pre-existing and healing overuse injury I had developed the previous year from too much running.)
Well, that was why I couldn't walk. Seems like my knee basically exploded inside me. I'm pretty appalled at the level of damage from what had seemed to be a benign jump from one boulder to another, but it seems most likely to me that I had a torn ACL already, from 7 years previous when I had popped through into a crevasse, torqued my knee into such an unnatural position and heard/felt a pop, and proceeded to pay an ortho specialist $300 to tell me I just had a sprain; in the years since I had a few occasions where the knee "gave out" briefly but it always seemed okay immediately after so I didn't give it much thought. Until now. It was the (probably already torn) ACL that gave out first and then as my weight continued to come down on my knee the rest was just a cascade of snaps and tears. Needless to say, I am in for a long haul recovery....again...
The ER at the Estes Park Hospital was characteristically empty when I arrived, and a nurse rushed to meet me with a wheelchair as soon as she saw me hop out of Nate's truck. I spent the next several hours filling out forms, being prodded, getting x-rays and an MRI, talking with the attending ER doctor, scheduling some surgeries, and texting my parents in the interim periods. The news was not good (bold are the main ones requiring surgery and long-term recovery):
Fracture of the posterior aspect of the lateral tibial plateau, predominantly a nonarticular cortical depression fracture, but there is also an osterchondral component involving the posterior articular surface.
Cartilage defect (approximately 12x4 mm) within the posterior lateral tibial plateau at the osterochondral fracture site.
Torn proximal ACL.
MCL and FCL sprains. No high-grade tear identified.
Large, displaced bucket-handle tear of the lateral meniscus with the handle displaced into the intercondylar notch, slightly greater anteriorly.
Vertical longitudinal tear of the peripheral posterior horn of the medial meniscus (ramp lesion).
Large hemarthrosis with posterior capsular tear and extensive hemorrhage and edema within the popliteal fossa.
Bone contusion of the anterior aspect o the tibial plateau involving the medial and lateral aspect and a smaller bone contusion of the posterior medial tibial plateau. Small osterochondral impaction fracture of the anterolateral femoral condyle at the condylopatellar sulcus and bone contusion of the upper peripheral lateral femoral condyle.
High-grade partial thickness tear of the mid substance of the quadriceps tendon at its patellar insertion measuring approximately 13 mm in length. The peripheral fibers, lateral greater than medial, are intact. (Note: This quadriceps tendon damage was likely a pre-existing and healing overuse injury I had developed the previous year from too much running.)
Well, that was why I couldn't walk. Seems like my knee basically exploded inside me. I'm pretty appalled at the level of damage from what had seemed to be a benign jump from one boulder to another, but it seems most likely to me that I had a torn ACL already, from 7 years previous when I had popped through into a crevasse, torqued my knee into such an unnatural position and heard/felt a pop, and proceeded to pay an ortho specialist $300 to tell me I just had a sprain; in the years since I had a few occasions where the knee "gave out" briefly but it always seemed okay immediately after so I didn't give it much thought. Until now. It was the (probably already torn) ACL that gave out first and then as my weight continued to come down on my knee the rest was just a cascade of snaps and tears. Needless to say, I am in for a long haul recovery....again...
RECOVERY TIMELINE (WITH PHOTOS)
Key: Days from injury
Days from surgery
|_Injury/
Helicopter/
Hospital/ Surgeries
|_Appoint./
Tests
|_Physio related
|_Other
DAY
0
12:05 pm, Thu,
Aug 20
Injury. Hurt knee near summit of Arrowhead.
1.
1. We wrapped my leg in a pack and I crawled from the summit to the first rappel anchor.
DAY
1
Fri,
Aug 21
Helicopter Evacuation.
2.
2. The hoist.
DAY
1
Fri,
Aug 21
Hospital. Estes Park Hospital.
3.
3. In the hospital filling out some paperwork....getting ready for some bad news....
Encounter Notes:
HISTORY: Knee pain and instability.
COMPARISON: Lower leg radiographs on the same day.
TECHNIQUE: T1 coronal. SE PD sagittal. T2 fs axial, sagittal, and coronal.
FINDINGS:
Osseous: A predominantly nonarticular cortical depression fracture of the posterior aspect of the lateral tibial plateau is present with a smaller component involving the articular surface. A shallow osteochondral impaction fracture of the lateral femoral condyle at the condylopatellar sulcus is present. A large bone contusion of the anterior aspect of the tibial plateau is present within the midline and involving the medial and lateral aspects. There is a small bone contusion of the posterior aspect of the medial tibial plateau and the inferior patella and the peripheral upper lateral trochlea.
Cartilage: An approximately 12 x 4 mm cartilage defect with a small portion of the underlying subchondral bone is present within the posterior aspect of the lateral tibial plateau at the fracture site. There is attenuation and increased signal within the anterolateral femoral condylar cartilage at the osteochondral impaction site. No deep surface defect within the medial femorotibial compartment is identified. There is mild swelling of the medial patellar cartilage on axial image 11. No deep surface defect within the patellofemoral compartment is identified.
Menisci: A large displaced bucket-handle tear of the lateral meniscus is present with the handle flipped into the intercondylar notch, greatest anteriorly. A large, peripheral, vertical longitudinal tear of the posterior horn of the medial meniscus (ramp lesion) is present.
Ligaments: The ACL is torn at its femoral origin. The PCL, MCL and FCL are intact with extensive MCL and FCL periligamentous edema. There also is evidence of a high-grade partial-thickness tear of the posterior aspect of the medial patellar retinaculum.
Tendons: A high-grade partial-thickness tear of the quadriceps tendon is present at its insertion on the patella. The lateral and to a lesser extent medial components are intact but the central portion is extensively torn best seen on sagittal image 15. The patellar tendon is intact. The iliotibial tract, biceps femoris and popliteus tendons are intact with mild edema at the popliteus musculotendinous junction. There is a strain of the origin of the lateral head of the gastrocnemius muscle. The plantaris tendon is not visualized and likely torn with a large amount of hemorrhage and edema in this location. The medial head of the gastrocnemius and pes anserine tendons are intact.
Joint: A moderate to large hemarthrosis is present with a posterior capsular tear. A trace of fluid is present within the semimembranosus-gastrocnemius bursa. Extensive edema is present within Hoffa's fat pad and the pancreas fat pads.
Neurovascular: Edema and fluid surrounds the popliteal neurovascular bundle. The visualized common peroneal nerve is unremarkable.
The findings were discussed with Dr. Daley.
IMPRESSION:
1. Fracture of the posterior aspect of the lateral tibial plateau, predominantly a nonarticular cortical depression fracture, but there also is an osteochondral component involving the posterior articular surface.
2. Approximately 12 x 4 mm cartilage defect within the posterior lateral tibial plateau at the osteochondral fracture site.
3. Torn proximal ACL.
4. MCL and FCL sprains. No high-grade tear identified.
5. Large, displaced bucket-handle tear of the lateral meniscus with the handle displaced into the intercondylar notch, slightly greater anteriorly.
6. Vertical longitudinal tear of the peripheral posterior horn of the medial meniscus (ramp lesion).
7. Large hemarthrosis with posterior capsular tear and extensive hemorrhage and edema within the popliteal fossa.
8. Bone contusion of the anterior aspect of the tibial plateau involving the medial and lateral aspect and a smaller bone contusion of the posterior medial tibial plateau. Small osteochondral impaction fracture of the anterolateral femoral condyle at the condylopatellar sulcus and bone contusion of the upper peripheral lateral femoral condyle.
9. High-grade partial-thickness tear of the mid substance of the quadriceps tendon at its patellar insertion measuring approximately 13 mm in length. The peripheral fibers, lateral greater than medial, are intact.
DAY 2
Sat,
Aug 22
Nate and Scott drive me and my car to Boulder.
DAY 2
Sat,
Aug 22
• Thigh circumference 36-49 cm, Calf 32 cm.
• Knee pretty swollen.
DAY 4
Mon,
Aug 24
Classes start at CU Boulder (thanks to Covid, all of my courses are online via Zoom).
DAY 4
Mon, Aug 24
Consult. With Dr. Khemarin Seng at Boulder Center for Orthopedics and Spine. Scheduled surgery for 10 days later. Given the go-ahead to hobble around. Goal is to get the swelling down and regain some mobility before surgery.
Encounter Notes:
History of Present Illness
Stephanie is a pleasant 37 yo female, presenting today for evaluation of her right knee after she was hiking out from climbing on friday 8/21/2020, missed a step, felt a pop in her knee and the "knee blew out," and the national guard had to come pick her up, went to estes park ED, had x-rays/mri's, and has been non-weight bearing in straight leg knee immobilizer.
pain is okay and taking no pain medications as long as she doesn't move it or weight bear,
hasn't been icing much due to the lack of pain, has been elevating a little bit,
RLE: moderate edema, no erythema/ecchymosis, ttp posterior/lateral tibial plateau, ttp superior patella/quad tendon insertion, nttp med/lat joint line, intact pain free straight leg raise w/ 5 degree extensor lag, flexion 0-80 w/ pain at end range, +lachman, guarded +pivot shift, unable to assess mcmurray's due to rom limitations, grossly nvid
Procedure Documentation
None recorded
Results/Interpretations
None recorded
Assessment and Plan
Assessment: right knee pain/injury s/p hiking fall, right knee mri review (acl tear, bone bruises of tibia/femur, lateral meniscus tear w/ bucket handle tear, medial meniscus tear ramp lesion, mcl strain, fcl strain, hemarthrosis), dr. seng recommended discontinue straight leg knee immobilzer, dr. seng recommended RLE WBAT & PT/hep/"prehab" for rom (rx sent to PT @ BCO), follow up with dr. seng on 9/1/2020 for rom recheck, or sooner w/ issues/concerns
Plan: I discussed the pertinent anatomy, etiology, and pathology of the patients issue with stephanie, advanced imaging was reviewed and discussed with the patient. Images and reports reviewed with patient within the context of their musculoskeletal issues. All pertinent questions were answered.
right knee mri impression:
1) fracture of the posterior aspect of the lateral tibial plateau, predominantly a nonarticular cortical depression fracture, but there also is an osteochondral component involving the posterior articular surface
2) approximately 12 x 4mm cartilage defect within the posterior lateral tibial plateau at the osteochondral fracture site.
3) torn proximal acl
4) mcl and fcl sprains, no high-grade tear identified
5) large, displaced bucket handle tear of the lateral meniscus with the handle displaced into the intercondylar notch, slightly greater anteriorly.
6) vertical longitudinal tear of the peripheral posterior horn of the medial meniscus (ramp lesion)
7) large hemarthrosis with posterior capsular tear and extensive hemorrhage and edema within the popliteal fossa
8) bone contusion of the anterior aspect of the tibial plateau involving the medial and lateral aspect and a smaller bone contusion of the posterior medial tibial plateau. small osteochondral impaction fracture of the anterolateral femoral condyle at the condylopatellar sulcus and bone contusion of the upper peripheral lateral femoral condyle
9) high-grade partial thickness tear of the mid substance of the quadriceps tendon at its patellar insertion measuring approximately 13mm in length. the peripheral fibers lateral greater than medial, are intact
- dr. robert leibold
dr. seng counseled that surgery is highly recommended for the meniscal injuries, and recommended for the acl tear, but we need to wait for the swelling/inflammation to decrease, and work on her range of motion.
dr. seng recommended cycling program/range of motion/heel slide & leg extension exercises, and obtain good strength/rom of the right knee, to allow inflammation/swelling to decrease and increase her range of motion
dr. seng counseled stephanie may wean from brace and crutches as tolerable, and that stephanie be wbat rle, all to allow her to start pt/rom/prehab
recommended ice every day, warm epsom salt soaks,
dr. seng counseled no cutting/pivoting/twisting, no bouldering,
dr seng recommended acl repair with hamstring autograft and med/lat menisectomy vs repair tentatively planned for 9/3/2020, and in office recheck with dr seng on 9/1/2020
follow up with dr. seng on 9/1/2020 for rom recheck, or sooner w/ issues/concerns
I discussed the risks, benefits, and alternatives to the treatment plan, answered all questions satisfactorily, the patient agreed with plan. Patient will call if anything worsens or if they have any concerns.
F/u: follow up with dr. seng on 9/1/2020 for rom recheck, or sooner w/ issues/concerns
60 minutes was spent in face to face contact, greater than 50% of which was spent discussing in coordination and care.
Case discussed with Dr. Seng who agreed with assessment and plan.
Protocols: acl injury/acl reconstruction in future possibly
DAY 4
Mon, Aug 24
• Hobbling slowly around the house in knee brace, 100% weight-bearing.
• Not too much pain.
• Swelling decreasing. Mobility increasing a bit.
• Icing on occasion and propping leg up while sitting down.
• Able to drive my car.
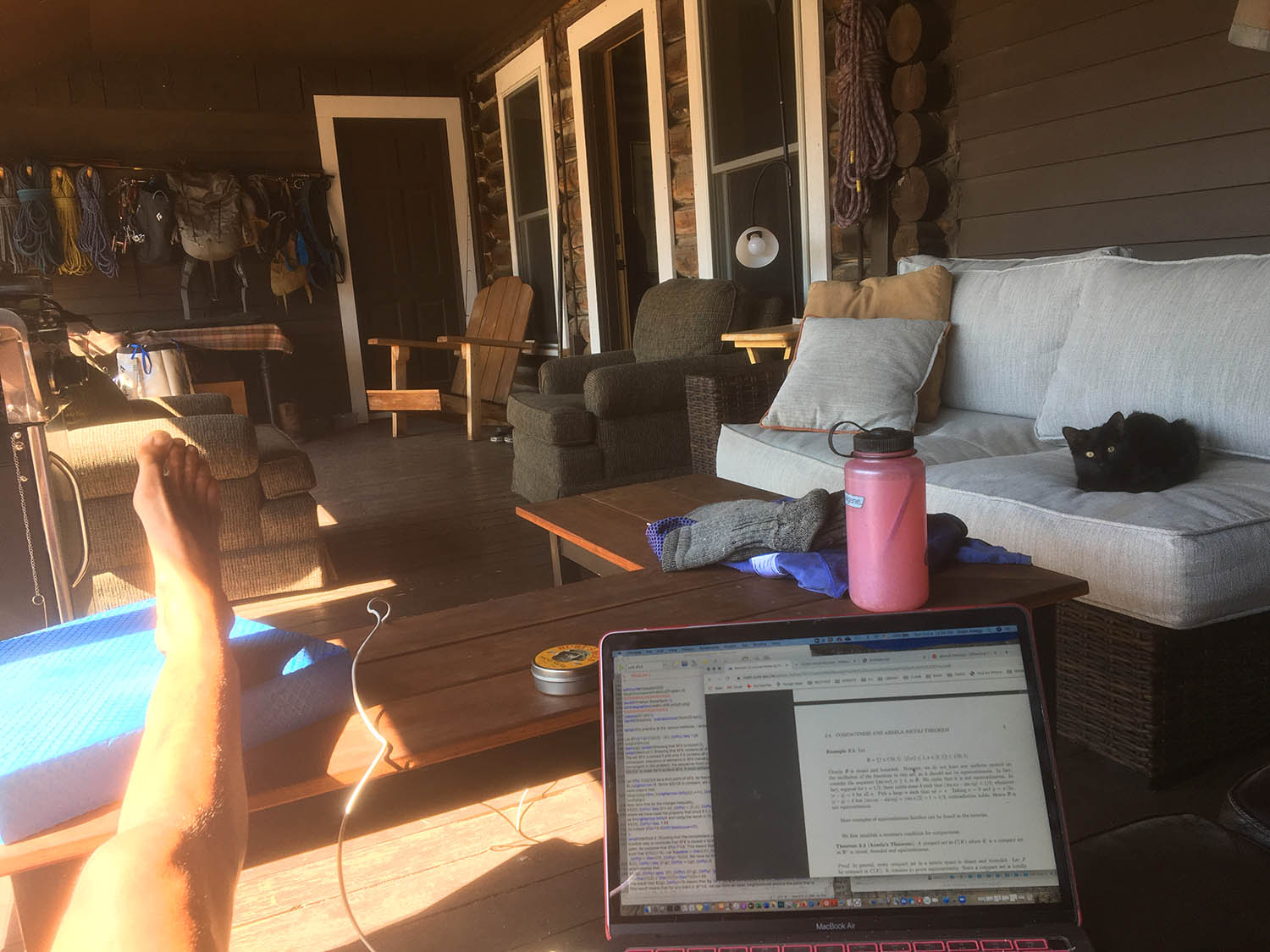
4.
4. Life is always better when you have a cat in your lap.
DAY 5
Tue, Aug 25
Numerical Analysis Preliminary Exam. Passed it but I'll try again in January to get a Research Pass.
DAY 8
Fri, Aug 28
Probability & Statistics Preliminary Exam. Research pass!
DAY 11
Mon, Aug 31
Pre-operative COVID Test. No COVID!
DAY 12
Tue, Sept 1
Pre-operative Consult. With Dr. Khemarin Seng at Boulder Center for Orthopedics and Spine. Admittedly, he did advise waiting another couple of weeks until surgery in order to gain even more mobility going into surgery, but I declined, not wanting to delay the start of my "recovery" any longer and feeling that my attempts to do phyiso at this stage would be much more half-hearted then they would be post-surgery.
Encounter Notes:
History of Present Illness
None recorded
Review of Systems
Patient reports no fever, no night sweats, no significant weight gain, no significant weight loss, and no exercise intolerance. She reports no dry eyes, no irritation, and no vision change. She reports no difficulty hearing and no ear pain. She reports no frequent nosebleeds and no nose/sinus problems. She reports no sore throat, no bleeding gums, no snoring, no dry mouth, no mouth ulcers, no oral abnormalities, and no teeth problems. She reports no chest pain, no arm pain on exertion, no shortness of breath when walking, no shortness of breath when lying down, no palpitations, and no known heart murmur. She reports no cough, no wheezing, no shortness of breath, and no coughing up blood. She reports no abdominal pain, no vomiting, normal appetite, no diarrhea, and not vomiting blood. She reports no incontinence, no difficulty urinating, no hematuria, and no increased frequency. She reports no abnormal mole, no jaundice, and no rashes. She reports no loss of consciousness, no weakness, no numbness, no seizures, no dizziness, and no headaches. She reports no depression, no sleep disturbances, feeling safe in relationship, and no alcohol abuse. She reports no fatigue. She reports no swollen glands and no bruising. She reports no runny nose, no sinus pressure, no itching, no hives, and no frequent sneezing.
Physical Exam
Patient is a 37-year-old female.
Procedure Documentation
None recorded
Results/Interpretations
None recorded
Assessment and Plan
ACL tear, lateral meniscus tear, medial meniscus tear ramp lesion, mcl strain, fcl strain, hemarthrosis-- proceed with r knee scope. ACL recon ALLOGRAFT, bilat menisectomies v. repairs. Work on stretching, begin PT post-op. FU post-operatively.
M presents to the clinic today for further discussion of R knee scope. ACL recon bilat menisectomies v. repairs. BSC. ROM check. She has some mild swelling and tightness in her hamstrings. She has some questions. She likes to hike and climb. She is inquiring about ALLOGRAFT
M's past right knee radiographs appear to indicate chondrocalcinosis.
exam with 3-95
mild effusion
+Lachman
better exam than last week.
R knee past MRI: acl tear, bone bruises of tibia/femur, lateral meniscus tear w/ bucket handle tear, medial meniscus tear ramp lesion, mcl strain, fcl strain, hemarthrosis
M's range of motion is better than previous visit, but still limited within its range. Her comfort with her knee appears better. I recommended waiting a couple more weeks in order to continue to improve her ROM, she would like to proceed sooner with treatment and risks with arthrofibrosis. . As stated previously I think she is a good surgical candidate for r knee scope. ACL recon, bilat menisectomies v. repairs. I explained the risks of surgery to M based on her limited ROM, because rehab and PT will be much harder if she lacks ROM. We discussed allograft vs. autograft. She elected to proceed with allograft. I answered all questions. She should continue stretching, stationary bike, FU post-op, begin PT post-op.
ACL recon
Allograft
meniscal treatment
25 minutes was spent in face to face contact, greater than 50% of which was spent discussing and coordinating patient care.
1. Complete tear, knee, anterior cruciate ligament - Right
S83.511D: Sprain of anterior cruciate ligament of right knee, subsequent encounter
PHYSICAL THERAPY REFERRAL -
Schedule Within: provider's discretion
Evaluate & Treat: post r knee scope. ACL recon ham auto, bilat menisectomies v. repairs, work on swelling and ROM
2. Bucket handle tear of lateral meniscus of knee - Right
S83.251D: Bucket-handle tear of lateral meniscus, current injury, right knee, subsequent encounter
3. Tear of medial meniscus of knee - Right
S83.231D: Complex tear of medial meniscus, current injury, right knee, subsequent encounter
4. Sprain of medial collateral ligament of knee - Right
S83.411D: Sprain of medial collateral ligament of right knee, subsequent encounter
MEDIAL COLLATERAL LIGAMENT INJURY: CARE INSTRUCTIONS
5. Hemarthrosis of right knee
M25.061: Hemarthrosis, right knee
6. Chondrocalcinosis of joint of right knee
M11.261: Other chondrocalcinosis, right knee
DAY
0 /14
(0 days from surgery)
(2 weeks from injury)
Thu, Sept 3
Knee Surgery. ACL repair via allograph + double meniscus repair.
5.
6.
7.
8.
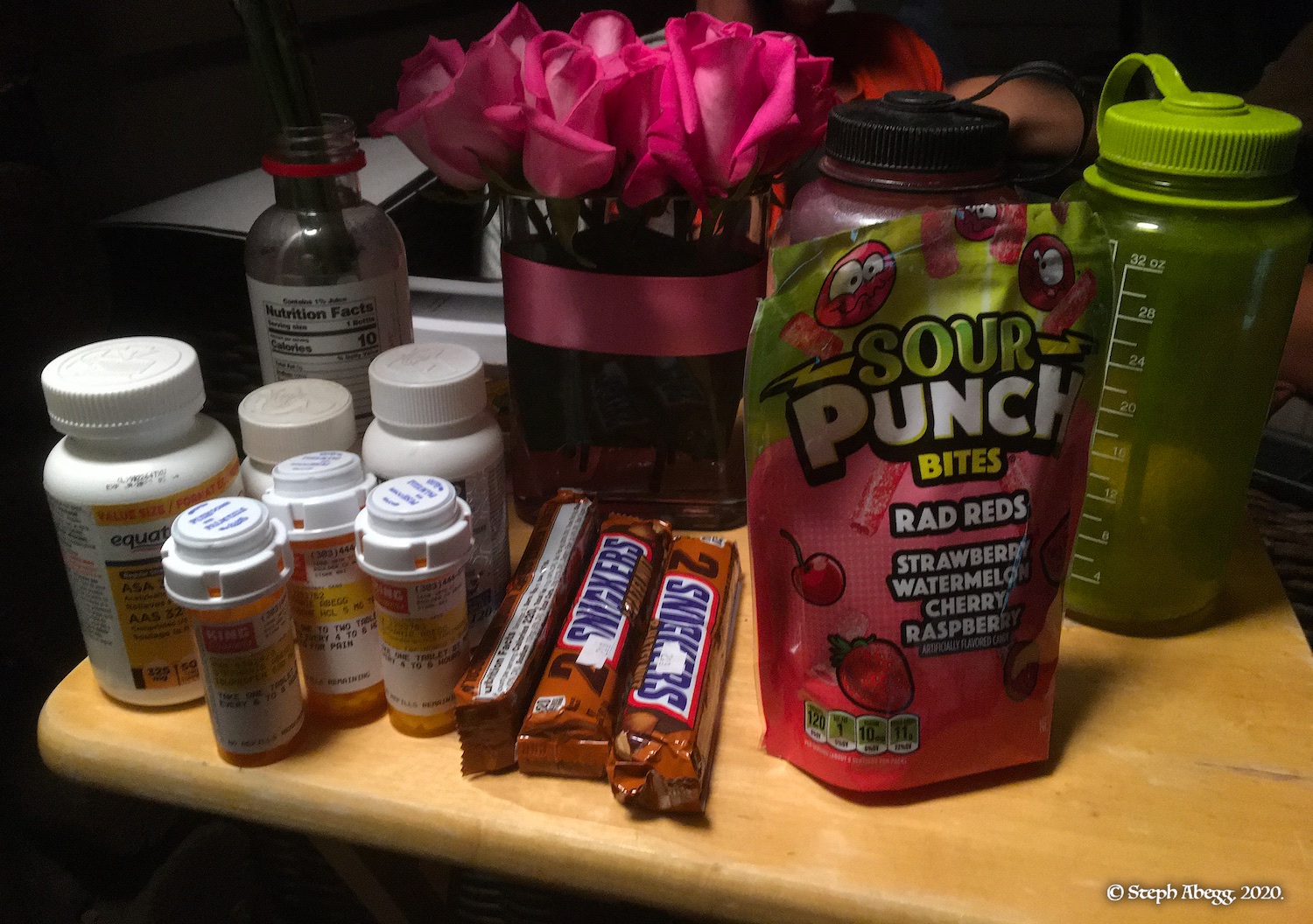
5. Covid-style waiting room. 6. Taken less than a day after surgery, working on some homework. 7. My pharmacy improved thanks to thoughtful friends Cassie and Taylor. As for pain meds, I ended up being able to keep the pain tolerable with just Tylenol and ibuprofen and hazelnut snickers. I'll save the two bottles of narcotics for my first aid kit. 8. It's great to have friends that understand.
DAY 2 / 16
(2 days from surgery)
Sat, Sept 5
• Allowed full weight bearing and bending leg 60° down from fully extended (bending limited due to meniscus repair).
• Hobbling slowly around the house in a cyborg knee brace without crutch support, 100% weight-bearing. Apparently typical ACL repair recovery timeline is to be on crutches for about a week after surgery, so already I am ahead of schedule, despite the meniscus repair to boot. That's a good sign!
• I am supposed to wear the knee brace for about 6-8 weeks from my date of surgery. Mainly it is to protect the grafts from an unexpected slip. But I may decide to take my chances and ditch the brace early in the interest of mobility and strength, depending on how the knee feels in these coming weeks.
• Munching Tylenol and ibuprofen and avoiding the narcotics.
• Icing on occasion and propping leg up while sitting down.
• My friend (who had an ACL repair a couple of years previous) told me "physio is magic" and that his main regret was not doing more of it. So I've already started doing minor PT (stretching, massaging, icing, propping) and have no plans to stop the PT until I'm back in the mountains again.
9.
10.
9. I was curious to see how the incisions were looking. 10. The fancy knee brace they gave me can be set to lock off at any angle. It's set to 60° for awhile.
DAY 7 / 21
(1 week from surgery)
Thu, Sept 10
Post-operative Follow-up. With Dr. Khemarin Seng at Boulder Center for Orthopedics and Spine. Stitches removed.
Encounter Notes:
Assessment and Plan
1 week s/p R knee scope. ACL recon ham allo, bilat menisectomies v. repairs. 9/3-- making good progress. Brace readjusted. Initiate PT at MedX with Dr. Scrivner. WBAT 0-60. Progress 5-6 degrees per week. FU 4 weeks
Stephanie presents to the clinic today for routine post-op evaluation for R knee scope ACL reconstruction ham allo, bilateral menisectomies v. repairs 9/3. She reports that she is doing well. The brace feels a little loose, but with the cooler weather coming she will be wearing pants more and doesn't necessarily mind.
Right knee:
There is a good resting attitude of the knee
skin looks clean, dry, healthy,
sutures removed
3-60
Intra-operative arthroscopic images reviewed
I am limiting her range of motion to 60 today. Increase 5-6 degrees per week. In 1 month she should be near 90 degrees ROM. She will begin therapy in Estes at MedX with Dr. Scrivner, ACL and meniscal repair protocol. WBAT. She should do heel slides daily. Can do upper body workouts now. May remove brace at night if she is a calm sleeper, if she is waking herself up with pain or wakes up in pain, wear brace to bed. From 6-12 weeks we can push past 90 degrees. FU in 4 weeks.
25 minutes was spent in face to face contact, greater than 50% of which was spent discussing and coordinating patient care.
11.
12.
11. Got the stitches removed 7 days after surgery.
12. Still some swelling. And calf is experiencing some atrophy (-1.5 cm of circumference so far).
DAY 7 / 21
(1 week)
Thu,
Sept 10
• Hobbling around doing errands (not just my apartment any more) in knee brace without crutch support, 100% weight-bearing.
• Still only allowed to bend leg 60°from horizontal and increase this by 5° per week.
• No pain medications needed. I don't really have any pain.
• Icing on occasion and propping leg up while sitting down.
• Swelling decreasing.
• Driving again. My knee feels fine to do so.
• Thigh circumference 36-46 cm (-3 cm), Calf 30.5 cm (-1.5 cm).
DAY 10 / 24
(1 week + 3 days)
Sun,
Sept 13
• Walked about 3.5 miles, with crutches to absorb about 20% of my weight on my injured knee. For short distances, I don't use crutches.
• I am walking carefully around my apartment without the brace. Gotta be careful not to trip but it feels nice to have the brace off and knee actually feels pretty stable for just walking around my apartment. This might have something to do with the fact that - unbeknownst to me - I had a pre-existing ACL tear for the last 7 years that caused my knee muscles to have to strengthen a bit.
13.
13. 3-mile walk. The red material is to cushion the crutch handles. Crutches aren't too comfortable after an hour straight....my fingers are going a bit numb from pinching of some nerve in my armpit....
DAY 12 / 26
(1 week + 5 days)
Tue, Sept 15
• Physio Appointment #1. With Rob Scrivner at MedX of Estes. Rob is a fellow climber and physiotherapist in Estes Park. He understands my goals of getting back to boulder-hopping, scree-sliding, drop-knees, and offwidths.
• Prescribed daily physio (Forward Ts, Planks, Step Downs and Step Ups, Leg Raises, Single Leg Stance, Passive and Prone Knee Extensions, Patellar Glides). I plan to do physio+walking for at least 2 hours every day, as I see it as my ticket to getting back to climbing by the spring.
• Some soreness after physio exercises. Lots of tightness trying to bend knee past about 70°. Main focus at the moment is straightening the leg fully and even hyperextend slightly. The fact that I am able to fully straighten (albeit with a bit of discomfort and difficulty) is apparently ahead of schedule for most ACL/meniscus recovery timelines. That's a good sign.
• Walking 3 miles (1 hour) a day in brace without crutches. I limp a bit in the brace, but I don't feel much pain or weakness in the knee.
• Haven't felt the need to ice the knee due to not much swelling or pain. • Have developed a seroma on one of my incisions. About a week after surgery, I noticed that one of my four incisions had a growing bump underneath. Google tells me this is called a seroma. A seroma is a collection of fluid that builds up under the surface of your skin. Seromas may develop after a surgical procedure, most often at the site of the surgical incision or where tissue was removed. The swelling and fluid may start right away, or may start collecting several weeks after surgery as it did in my case. Minor, small seromas like mine don’t always need medical treatment. That’s because the body may naturally reabsorb the fluid in a few weeks or months. So I guess I will just wait and see. I have bigger priorities at the moment. See photo below. (Update: It took about 6 weeks for the seroma to dissipate to the point where it was barely noticeable.)
14.
15.
16.
17.
14. Awesome to have a physiotherapist as psyched as me to get me back to climbing as soon as possible. 15. Doing "passive knee extensions" with weight as I watch a lecture to try to get my leg fully straight.
16. Daily 3 mile walk. No crutch support now. Just the cyborg knee brace. 17. Seroma.
DAY 18 / 32
(2 weeks + 4 days)
Mon, Sept 21
• Physio Appointment #2. With Rob Scrivner at MedX of Estes.
• Rob was pleased with my improvement over the last week. He recommended continuing the same exercises for another week, but adding in some 70° squats and making the balance exercises more challenging by using a foam pad or closing my eyes. He also recommended massaging the seroma to try to get it to break up and get re-absorbed by my body. I did this for a day or two before getting bored of that exercise (my diligence on physio is clearly a bit selective.)
• The 3 mile walk and going up and down stairs is getting easier by the day. The progress gives me hope and motivation.
• No issues (pain, stiffness, etc.) straightening and even hyperextending the leg.
• Thigh circumference 36-47 cm (-2 cm from normal but +1 cm from 2 weeks previous), Calf 31 cm (-1 cm from normal but +0.5 cm from 2 weeks previous). Looks like atrophy has been pretty minimal due to the fact I got back to weight-bearing quickly.
• I officially stopped wearing the brace 3 weeks after surgery. This would be a bit too soon by most protocols (some protocols suggest wearing a brace up to 2 months following an ACL+meniscus repair) but my knee feels stable and strong, isn't swollen or painful, and my walking has a much more comfortable and normal gait without the brace. The main reason for the brace is to protect my vulnerable ACL graft and meniscus repair against an unexpected trip or biker careening into me on the walking path. Given how stable my knee feels and how nice it feels to walk without the brace, I've decided to take my chances. I hope I don't regret this decision.
18.
19.
20.
21.
18. My daily 3 mile walk. If I am going to take the risk of not wearing a brace, I am at least going to make the terrain as flat and predictable as I can. 19. I've added stairs to my daily routine. I was able to start going down stairs (with difficulty) at about 2 weeks after surgery, and by 3 weeks after surgery it is getting pretty easy although there is tightness in the injured (right) knee when I step down with my good leg and my right knee has to bend. 20. Walking without the brace, 3 weeks after surgery. Besides for a slight limp, the knee behaves fairly normally for walking on a flat path at just over 3 mph.
DAY 26 / 40
(3 weeks + 5 days)
Tue, Sept 29
• Physio Appointment #3. With Rob Scrivner at MedX of Estes.
• Rob was pleased with my progress, and gave me a couple of additional exercises to do and the go-ahead to start using some weight machines, as long as I continued to not bend the leg past 90° (again, not wanting to overload the meniscus repair is the reason for this, rather than the ACL repair).
• Rob is going on a climbing trip for a few weeks, but I can continue with my daily physio routine and weights and hopefully be ready to start bending past 90° by next appointment with him in a few weeks. I loaned him my Needles (California) guidebook and hope to hear of some awesome climbing he did on his trip.
• After a week in the gym, thigh circumference 36-49 cm (back to normal), Calf 31 cm (-1 cm from normal still). So I've seemed to have beat the atrophy. I'll maintain the gym workout sessions to keep my body and knee strong, so all I am waiting for is the ACL graft and meniscus repair to become strong enough to get back to more enjoyable and calorie-burning activities. And a good way to prevent re-injury in the future will be keeping everything else around the knee strong.
• I devote about 3 hours a day to physio: 1.5 hours of weights (arm, core, and legs), 20 minutes of stretching and balance, and 1 hour dedicated to a walk on a paved path. All without a brace, which I stopped wearing 3 weeks from surgery. I know 3 hours per day of physio sounds a bit excessive, but without climbing I need to focus my non-school energies on something, and one of those somethings has become physio so I can get back to climbing as soon as physically possible. How fast can I get back? Let's see! (is my motto every day) I feel I am staying ahead of the recovery timeline, so it seems my rehab efforts have been beneficial so far.
• Still feeling far from being able to jog down scree slopes, hop from one boulder to another, drop knee my way through a climbing move, or thrutch up an offwidth, but those are the goals....
22.
23.
24.
25.
26.
27.
22. Leg press (quads, hamstrings, glutes). 23. Knee extensions (quads). 24. Recumbent bike (I cannot use a normal upright stationary bike quite yet since I cannot bend knee more than 90°). 25. Stairmaster! 26. The weekend. Wish I was climbing, life is a bit more boring and sedentary these days, but still pretty pleasant. 27. I was going to caption this photo with something like "drinking my knee injury days away" but the true story is I ended up with a tooth abscess/infection, and the few days leading up to a fast-tracked root canal put pain into perspective and caused me buy my first bottle of whiskey. I actually quite liked it, but kept the rest of the bottle for the next root canal.
DAY 47 / 61
(6 weeks + 5 days)
Tue, Oct 20
• Physio Appointment #4. With Rob Scrivner at MedX of Estes.
• For the last few weeks I had been gradually increasing the bending of my knee up to 90° (not wanting to stress the meniscus repair is the main reason I haven't focused on bending much). My knee is pretty stiff once I try to bend past 90°, but Rob instructed me to bend it as far as I could and I was able to bend to 115°.
• It seems that 90-100° is about what you need to be able to bend to make a full pedal circle on a stationary bike. Yay, progress and another way to exercise and work on getting rid of the stiffness in my knee.
• Rob added hamstring stretches as well as a terminal knee extension resistance band exercise to my physio regime to strengthen the hamstrings to be able to more easily lock off (slightly hyperextend) my leg.
• I'd also started to notice a bit of clicking of my knee-cap as I've been pushing my mobility. In fact, when Rob was bending my knee we could actually see the knee-cap shifting during the clicking noise. It's likely due to tightness of the patella's side stabilizing ligaments, so Rob also have added patella mobilization massages to my daily regime. At least this one I can do as I attend my Zoom lectures. In fact, I spend many of my lectures stretching and massaging my knee, something that has been made much easier due to the fact that school has gone online this semester (due to COVID-19).
• The seroma I had developed about a week after surgery has become much smaller and will probably be completely gone within a couple of weeks.
28.
29.
30.
31.
32.
33.
34.
35.
28. Now that I can bend my knee to 90° I have incorporated the stationary bike into my daily exercise/physio routine. 29. This is as far as I can bend it just under 7 weeks from surgery, around 115°. 30. Terminal knee extension resistance band exercise. 31. Doing patella mobilization as I study. 32-33. Estes Park traffic jam! (As seen from my morning walk after a physio appointment with Rob.) 34-35. Even Fred and the campus mascot are wearing face masks these days.
DAY 54 / 68
(7 weeks + 5 days)
Tue, Oct 27
• Physio Appointment cancelled due to evacuation of Estes Park because of East Troublesome fire, which had jumped the divide and was threatening to burn down RMNP and Estes Park. Fortunately a snowstorm had moved in over the weekend and calmed the flames so disaster never struck Estes.
DAY 54 / 68
(7 weeks + 5 days)
Tue, Oct 27
8-week Follow-up Appointment. With Dr. Khemarin Seng at Boulder Center for Orthopedics and Spine. "Keep doing whatever you've been doing!" was the main advice Dr. Seng had for me. He even mentioned that perhaps I could start jogging or toproping by December.
Encounter Notes:
Assessment and Plan
7.5 week s/p R knee scope. ACL recon ham allo, bilat menisectomies v. repairs. 9-3-2020-- Continue regaining full ROM, use stationary bike daily, massage/foam roll scar tissue, consider BFR. Progress 5 degrees flexion per week. FU in 5 weeks.
Stephanie presents to the clinic today for routine post-op evaluation for R knee scope ACL reconstruction ham allo, bilateral menisectomies v. repairs 9/3. She reports that she is doing well and has been doing physical therapy once per week in Estes with her climbing friend. The knee feels stable, she has not been wearing the brace for a couple of weeks. She reports that she puts in 3 hours of physio per day. She can flex her knee slightly past 90 degrees without loading it.
Right knee:
Teardrop crease VMO looks good
no swelling
full extension
120 flexion
negative Lachmann's
neg pivot shift
I informed Stephanie that she has made significant progress since her previous visit and is doing very well. Stephanie will focus on regaining full ROM, use a stationary bike, do banded exercises (monster crab walks, single leg lifts), and perform isometric exercises. By 12 weeks my goal for Stephanie is that she will have significant ROM, muscle activation, and that she will be ready to load the knee in squats. I informed her that she will have to wait until approx. 12 weeks for tissue to scar in appropriately. I informed her that the clicking that she has been feeling is a result of the beginning of the scar tissue formation. She will continue massaging scar tissue area, will work on progressing 5 degrees in flexion per week, and will continue to do daily heel slides. We discussed BFR, I explained the activity, risks, benefits, and expected outcomes. She was given a BFR script today. I informed her that at the next visit we will discuss if she can begin to run, hike, snowshoe, and/or in-door climb. Patient understands and agrees with plan. All questions were answered thoroughly. Follow up in 5 weeks for recheck at the 3 month mark.
doing well
progress PT
consider BFR
fu in december to discuss light indoor climbing
25 minutes was spent in face to face contact, greater than 50% of which was spent discussing and coordinating patient care.
DAY 61 / 75
(8 weeks + 5 days)
Tue, Nov 3
• Physio Appointment #5. With Rob Scrivner at MedX of Estes.
• I am religious to my daily 3-hour exercise+physio routine. I wake up most mornings at around 5 am to get it all done before school and other life events. At this point, my routine involves (1) 30 minutes on the stationary bike, (2) 20 minutes on a stairmaster or elliptical, (3) 1 hour 20 minutes of weights for both legs and arms, (4) 20 minutes of stretching/massaging/balancing/physio, and (5) 30 minute walk. Dedication to this daily routine is easy when getting back to climbing is the prize.
• Rob gave me some more physio-specific exercises to do (band pulls and quad stretches to increase knee flexion, monster walks, balance ball, side planks).
• Rob recommended starting to increase the weights on the machines but to do fewer reps. This would give some time to do the extra physio-specific exercises. I might also start to walk a little less if I need more time for phyiso-specific exercises, although I like to be outside and that gives me a way to be outside everyday for a bit.
• Rob had be jog on the treadmill for a minute. It felt great. At my previous appointment with my surgeon, my surgeon had mentioned "maybe starting to jog a bit by December" and this seems likely. But for now, I've been starting to use the elliptical on some days. Interesting to think that I was initially told I should be in the knee-brace until about 8 weeks from surgery, but I feel a pretty long way from needing the brace anymore. For me, the risk of the early exit from braceland was worth the reward.
• I can bend my knee to 120° before feeling discomfort. We got it as far as 126° after massaging the quad a bit. 90° was the goal by now so I guess I am ahead of schedule. So far I am only loading it at 90° or less.
• Rob asked me to come up with a climbing goal for the upcoming summer that we can work towards. I told him it was Ariana on the Diamond. A 6-pitch 5.12a route with a rugged approach and descent is probably a bit unrealistic but I would love for my knee and body to be back at that by August or so. Rob says he will help develop a rehab/training plan specific to my climbing goals. Nice to have a physiotherapist on the same page!! (July 28 2021 update: I actually achieved my unrealistic goal after all!. I climbed Ariana. Click here to see the trip report.)
36.
37.
38.
39.
40.
36. 120° is as far as I can bend it comfortably. 37. Some more physio exercises. 38. One-leg balancing on the Bosu ball. I've no problem staying balanced for over a minute at a time. It's equally easy (or hard, depending on the task) to balance with my right leg as with my left at this point. 39. On the elliptical. 40. Knee looks pretty normal at this point.
DAY 68 / 82
(9 weeks + 5 days /
2 months + 7 days)
Tue, Nov 10
• Physio Appointment #6. With Rob Scrivner at MedX of Estes.
• I can bend my knee to 135°, 9° more than the previous week. I am still not loading it much past 90°. I feel the daily exercised bike is probably helping the most with being able to bend my knee with minimal tightness in the joint.
• Rob added 10 minutes of treadmill (4x 2.5 minute intervals) and rowing machine (unlimited) to my list of exercises. I'll probably be reducing the amount of time I spend on the elliptical or walking outside (it's getting cold out now) to fit these into my daily routine. Feels nice to be able to start to sweat again.
• Rob is also working on a hang board routine I can incorporate into my daily routine. I've never been much for hangboarding since I'd rather be out climbing, but everyone swears by it and this is as good a time as any to get into it. Would be great to come out of this injury being able to hang onto 5.11/12 crimpers!
• Most of my physio is for my right knee, but Rob has given me a few exercises to do for my left leg/ankle, to see if I can improve its strength so my foot will more naturally face forward like a normal foot. (In 2010, I had a rather severe tib/fib injury and a MRSA infection that caused the metal hardware to be removed prematurely, and as a result my foot healed 19° misaligned. I opted out of the re-break to fix it, since it would have required external fixation and another 6 months (added to the 9-10 months already) on crutches. Although I have no regrets for opting out of the re-break, my foot has always cocked outwards and resulted in a bit of an abnormal gait. But never too late to see if I can get some improvement!)
• I bought a Bosu ball on Amazon for $60 so I can do balance exercises at home. Also makes a nice seat.
• I installed a hangboard above my bathroom doorway. See photos below.
41.
42.
43.
44.
41. Row machine. 42. Running on the treadmill! Just for 5 minutes at a time for now. 43. Inspired by Rob's addition of hangboarding to my physio routine, I finally got around to mounting my hangboard in my apartment. I mounted it on a doorway pullup bar. 44. A bit of internet research shows lots of DIY ways people have mounted hangboards to pullup bars. I followed the technique posted here, and it worked superbly. All I needed was a drill and a few supplies easily acquired at the hardware store. The process went as follows: To mount the hangboard on the pullup bar, I mounted the hangboard on a piece of wood, and then mounted the wood on the pullup bar via 5-inch long threaded pipe nipples inserted into the pullup bar itself, with flanges at the ends attached to the board (see photo). I found the pipe nipples and flanges in the plumbing aisle at the hardware store. Unfortunately my apartment has no doorframes (needed to rest the pullup bar on) so I had to screw in four thick screws. Don't tell my landlord.
DAY 75 / 89
(10 weeks + 5 days /
2 months + 14 days)
Tue, Nov 17
• Physio Appointment cancelled since Rob caught COVID-19. Fortunately, this illness has a rather high rate of survival despite what the media might lead you to believe.
DAY 84-86 / 98-100
(12 weeks + 0-2 days /
2 months + 23-25 days from surgery)
Thu-Sat, Nov 26-28
• Thanksgiving climbing trip to Shelf Road. I was expecting to attempt to climb one route, have the knee feel kinda tweaky, and spend the rest of the trip belaying. But I ended up climbing 5-6 pitches on toprope a day, mostly 5.9-5.10 with a couple of 5.11's I struggled on, too cautious to do any weird movement of small footholds with my right foot. Still a ways to go to get back to where I want to be but so nice to be back on the rock!
45.
46.
47.
48.
45. Hiking with a 30 lb pack Knee felt just fine. 46. Nice to be back on the rock! 47. Climbing this sort of stuff seems like good physio. 48. Not a bad office.
DAY 89 / 103
(12 weeks + 5 days /
2 months + 28 days)
Tue, Dec 1
• Physio Appointment cancelled since I had to study for a final exam. I did mange to fit in a few hours of walking and my own physio, as usual. • I have started to hike an hour a day on the trails around the Flatirons. I wear a pack filled with 35lbs of weights. I don't wear a knee brace as the cyborg one its quite uncomfortable to hike in and any other brace is probably not enough to really prevent injury if a force was actually great enough to injure it. I suspect I am pushing the limits of what might be a good idea to do, but I am willing to take the risk in the interest of progress and sanity.
• The popping/clicking of my knee cap has stopped. I think the patellar glide exercises and biking really helped loosen up the scar tissue that was causing the clicking.
• My most noticeable knee issues are that I cannot bend it fully so that the back of my calf can hit my thigh (I feel pain and stiffness when I try) and it does not hyperextend much like my good knee can. Also, I cringe at the thought of twisting, squatting, stemming, drop-knees, heel-hooks, high-steps, or off-widths, so there's still a fair bit of weakness and instability there, as would be expected at slightly less than 3 months from surgery.
49.
50.
50.
49. Trail. 50. Hiking. 51. My backpack is loaded with weights.
DAY 93-4 / 107-8
(3 months + 2-3 days from surgery)
Sat-Sun, Dec 5-6
• Cragging (Upper Kenny Mountain & Kenny Ridge) with Nate, Bernard, and Scott! Moderate face up to 5.10 A0 face climbing is my zone right now. Feels so good to be getting out again with my favorite people to hang out with!
51.
52.
53.
54.
55.
56.
57.
51-53. Approach. 54-56. Climbing! 57. Squeezed in a day of gym climbing a couple of days later.
DAY 98 / 112
(14 weeks /
3 months + 7 days)
Thu, Dec 10
3-month Follow-up Appointment. With Dr. Khemarin Seng at Boulder Center for Orthopedics and Spine. Dr. Seng watched my gait with and without high-stepping and had me stand on one leg. Pretty easy stuff for me at this point. He said I am cleared for all "in-line" activities (such as biking, hiking, jogging, and certain climbing). At my current rate of progress, he sees me as being able to get back into what he calls "at-risk" activities by the 6-month mark, which would be early March, which bodes well for the spring and summer climbing season. The next few months will focus on building up strength in the gym and starting to do squats. Of course I will also keep hiking, jogging, biking, and climbing. I did mention I had climbed a bit already and he didn't seem too concerned with that fact but told me to be careful with what sort of movements I do.
Encounter Notes:
Assessment and Plan
3 months s/p R knee scope. ACL recon ham allo, bilat meniscal repairs. 9/03/2020--
feeling well. has been hiking with full backpack around mesa trail
no interval trauma
wants to climb the diamond in august 2021
went climbing without any problems
exam with neg lachman. neg pivot shift. 3-150 flexion. no swelling.
normal gait. normal heel toe walk. strong and stable single leg squat
she wants to get back in the the CU gym. she is happy that she had surgery
fu in 3 months and we can discuss at risk knee sport.
DAY
101 / 115
(3 months + 10 days)
Sun, Dec 13
• First time out winter hiking. Hiked up to Chasm Lake junction to take a peek at the Diamond. Was a sunny day but windy. Knee felt great. No knee brace. It seems as if my goal of being Diamond ready by summer is not so far-fetched.
58.
59.
60.
61.
58. Blustery hiking. 59. Diamond in distance. 60. Knee photo. 61. Nate found some dry rock!
DAYS
111-21 / 125-35
(3 months + 20 days
- 4 months from surgery)
Wed, Dec 23 - Sat, Jan 2
• Winter Break trip to Cochise Stronghold! Before I injured my knee in August, this had been the Winter Break plan. But then with my knee injury and my surgeon telling me no "at-risk" activities for 6 months, I figured the Cochise plan (which would be at slightly less than 4 months from surgery) wouldn't happen. But when my religious PT led my knee to start to feel pretty good by about 3 months in, the draw of warm sunny granite was too much, and Nate and I decided to go for it. I would just be careful with the knee. No leading, falling, stemming, drop-kneeing, or boulder-hopping for me. The risk of climbing with a still-healing 4-month-old ACL graft and meniscus repair was a risk I was willing to take. It was an awesome trip: 10 days of climbing and 14+ routes in the Stronghold, ranging from 5.6-5.11. As far as my knee went, it felt stronger and more confident by the day and I had no issues. A good summer alpine climbing season looks pretty feasible at this point. Click here to go to trip report!
62.
62. Me climbing a sea of sunny chickenheads at Cochise Stronghold.
DAY
129 / 143
(4 months + 7 days)
Sun, Jan 10
• First lead since the knee injury! Cackle Crack, a 5.8 crack at Lumpy Ridge.
63.
63. Me leading Cackle Crack.
DAY
130 / 144
(4 months + 8 days)
Mon, Jan 11
Numerical Analysis Preliminary Exam. Attempt number two (the first attempt had been five days after my knee injury, so I recall being in a fair amount of discomfort). Hope I get a Research Pass this time...or did I do too much climbing and too little studying over the break?...(Update: Research Pass!)
DAY
144 / 158
(4 months + 22 days)
Mon, Jan 25
• Physio Appointment #7. With Rob Scrivner at Alpenstrong Physical Therapy in Estes Park.
It has been over 2.5 since my last official physio appointment. Rob co-founded a new physiotherapy outfit (Alpenstrong Physical Therapy) in Estes Park in late 2020, and unfortunately my insurance does not cover me there. Although I am pretty good at undertaking my own physio and exercises, I do see benefit to having some guidance, especially from a fellow climber who completely understands my goals, so I have decided to see Rob once a month to get some tips and exercises for pushing my knee safely. As a fellow climber, he understands what I want to achieve out of my knee and is helping me get there.
• Rob gave me some exercises to do to work on the tightness of my knee. He also gave me some side-to-side and 90° jumping exercises to start to focus on lateral and twisting strength.
• The rest of this post contains some update notes on my recovery since my climbing trip to Cochise over winter break.
• I have been putting in 2-3 hours each day of physio+exercise. Pretty much the norm for the last 20 years of life so it's not a hard routine to stick to.
• Ever since returning home from the Cochise climbing trip, I have added jogging 30-40 minutes a few times a week to my routine. It feels great to be able to jog again, and I would do it every day, but I want to ease back into it.
• School has started back up with vengeance so I have less time for hiking in the Flatirons in the mornings, but I have increased my pack weight to 40 lbs when I do manage to fit in a hike. That's one way to make a climbing pack feel light!
• I have resumed cragging on weekends, not really planning approaches or climbs around my knee anymore. Even so, I am not yet leading regularly.
• As far as my knee goes, it feels pretty strong and I don't generate any soreness or swelling by my activity level. However, it's definitely not yet 100%. I know the grafts and meniscus repairs are still healing, so I avoid any twisting, squatting, jogging down trails, or boulder-hopping. I still experience stiffness and mild discomfort for two things: (1) weighting the knee with my body weight and hyperextending it slightly, and (2) trying to bend it fully (I cannot quite bend it all the way so that my heel touches my butt). I suspect that these are mostly a result of the meniscus repair (and the fact that I have had to avoid bending too much) than the ACL. Now that I am about 4.5 months since the surgery, I can baby the meniscus a bit less, so Rob has given me some exercises to start to work on this stiffness. (Update: After 2 weeks of doing daily knee-bending exercises, I am able to touch my heel to my butt.)
• More and more often I go about a day without thinking much about or favoring the knee.
64.
65.
64. New physio exercises from Rob. 65. This one is to help me be able to bend my knee fully again.
DAY
175 / 189
(6 months - 1 week)
Thu, Feb 25
6-month Follow-up Appointment. With Dr. Khemarin Seng at Boulder Center for Orthopedics and Spine. My knee has been feeling pretty good and my activity level is pretty much back to normal, so the main thing I was curious to ask Dr. Seng about was the status of the repair. He said that at this point an ACL graft and meniscus repair will be about 60-70% healed, and probably close to 90% or more healed within a year. If I were a football player I'd probably not yet be back in the game yet, but climbing and hiking is much less sudden pivots and twists. Dr. Seng said strength training (squats, leg presses, hiking with weight) is the best thing I can do to avoid reinjury of the still-healing tissue; fortunately, I do a lot of this and had no plans to stop until summer climbing season. His last piece of advice was to "Go out and have fun and just be careful!"
Encounter Notes:
Assessment and Plan
6 mo s/p right knee scope w/ ACL recon ham allo, bilat meniscal repairs 9/03/2020-- Doing well. Be smart and have fun. Lower-body/core exercise 2-3x weekly. Strengthening. FU 6 months.
Stephanie presents to the clinic today for a recheck of her right knee ~6 mo s/p R knee scope. ACL recon ham allo, bilat meniscal repairs 9/03/2020. She states that she is doing well. She has been working on strengthening and last bit of end ROM. She checks in with her physical therapist once a month. She is back to her normal activities for the most part. Has no complaints. Has been running 45 minutes per day and climbing for the past 2 months. Has not tried any twisting yet, but the knee hasn't felt painful or off.
feels stable, continues to climb and run without issue.
Right knee exam:
good teardrop
negative lachman's
negative pivot shift
2-160
incisions look great
6 mo s/p R knee scope ACL recon ham allo, bilat meniscal repairs
Stephanie is doing well. I informed her that it will take 12 months to get to 90-100%. Strengthen quads, glutes, hamstrings, and core. Add lower-body/core driven exercises 2-3x per week including squats, deadlift, leg press, and lunges. Resume or increase normal activities. Follow up in 6 months for recheck.
Follow up 6 months.
DAY
194 / 208
(6 months + 13 days)
Tue, Mar 16
• Physio Appointment #8. With Rob Scrivner at Alpenstrong Physical Therapy in Estes Park. It had been nearly two months since my last appointment with Rob. I had been religious with the exercises he had given me and it was time to check in, chat about climbing, and get some more physio exercises to do to start to push the strength and start doing some more dynamic stuff with the knee (like jumping).
• I've pretty much returned to full activity (running long distances, hiking, climbing, snowshoeing,....) and my legs are feeling stronger than ever due to weight work in the gym, but I still feel some stiffness in the knee joint and my knee-cap clicks on occasion. Rob suggests that the patellar mobilization exercises (one of the few exercises I have been slacking on) is probably my best way to expedite the process of overcoming the stiffness.
66.
67.
68.
69.
66. New physio exercises from Rob! 67. Single leg jumps onto my right knee. 68. Stepping up and controlled lower back down. 69. Getting ready for some knee drops....
DAY
242 / 256
(8 months)
Mon, May 3
• I haven't updated this page in awhile with my recovery progress, so I thought the 8-month-from-surgery mark would be a good time to do so. I've maintained my religious daily physio and exercise routines, and basically by now I am back to normal activity and my body and knee feel as strong as usual for mid-spring. There is a little stiffness in my knee still when I fully bend or extend it, but no pain and no weakness; I can run, hike, and climb as normal. I still do find myself favoring the knee for descents on rough terrain or hopping across creeks or between boulders, but that's a minor inconvenience. I do not wear a knee brace and find no need to do so. I am back to leading on rock again, although still lacking a bit of confidence with more committing right knee intensive moves or high steps with the injured knee. My last final exam was today, and my summer semester has begun. For the next few months, I plan to study for an important preliminary/comprehensive exam as well as have another great alpine climbing season! I don't plan to be held back much by my knee, other than to be a bit more deliberate about resting (good opportunity to study math anyway...) between big days out in the mountains instead of going hiking or running. Nice to be back in action!
70.
70. Leading at Lumpy Ridge.
DAY
303 / 317
(10 months)
Sat, July 3
• Alpine climbing season is in full swing and my knee feels great, pretty much normal at this point. No obvious stiffness and I hike and climb without favoring it.
71.
71. Me high on the Diamond.
DAY
351 / 365
(1 year from injury)
Fri, Aug 20
• One year from the injury! Apart from one more update from my 1-year appointment with my surgeon, this will be my final update on my knee. My right knee feels just as strong and mobile as my left knee at this point, apart from just a little stiffness at full bending and extension (which could probably be resolved if I got back into doing physio regularly, but my physio this summer has just been climbing, running, and hiking). Adventuring this summer was not restricted in the slightest by my knee, and it was weather that caused more rest days than I would have wished for. I climbed in the Black Canyon, Fremont Canyon, Vedauwoo, Mt. Evans, several objectives in RMNP including four ascents of the Diamond, Needles in South Dakota, Devil's Tower, Ten Sleep, Wind Rivers, and more. For a list of climbs I did since my knee injury go to my 2021 Trip Report Chronology.
DAY
355 / 369
Tue, Aug 24
Applied Analysis Preliminary Exam. Hard.
DAY
364 / 378
(1 year from surgery)
(1 year + 2 weeks from injury)
Thu, Sept 2
1-year Follow-up Appointment. With Dr. Khemarin Seng at Boulder Center for Orthopedics and Spine. A year ago on this date I was just about to get knee surgery and the near future was looking pretty bleak. But here I am a year later and been back to normal activity for awhile. And even with the injury, it was a pretty good year of my life. I thanked Khemarin for a surgery well done.
Encounter Notes:
Assessment and Plan
12 months s/p right knee scope w/ ACL recon ham allo, med + lat meniscal repairs 9/03/2020. Doing very well -- Proceed with normal activities and climbing, avoid falls -- FU in 12 months
Stephanie presents for a recheck of her right knee ~12 mo s/p R knee scope w/ ACL recon ham allo, bilat meniscal repairs 9/03/2020. She is doing well. Slight stiffness on left knee extension and slight stiffing full bending. She has been climbing (climbed the Diamond 4 times) with no complaints.
She is on her 3rd year of her PhD work.
Right Knee:
- Full extension
- 160 flexion
- Negative Lachman's
Left Knee:
- Grade I Lachman's
- Mild pivot glide
- 150 flexion
- I am pleased with Stephanie's recovery progression.
- I would spend 30% of week focusing on knee strengthening and rom.
- Timeline of healing of her right meniscus is 9-12 months.
- Two metrics she can look for healing of meniscus: objective imaging studies such as ultrasound or MRI or she can base it clinically by noting the function, feeling, ability to pivot/cut/twist.
- Continue climbing, running, bouldering as needed. Avoid falls.
- FU in 12 months, update every year via in-person, phone calls, of how knees is doing.
avid climber, might send climbing pictures
doing very well
FU in 12 months
1. History of reconstruction of anterior cruciate ligament tear
Useful beta. Updated route information. Corrections. Historical notes. Interesting facts. No fluff please. Please do not put links in your comment, as my spam filter will filter those comments out.